
Navigating Global Complexity: Applying ICH E17 to Modern Clinical Trial Biometrics
Clinical trials are no longer local experiments with global ambitions. Increasingly, they are global evidence systems from day one. Sponsors need data that can support regulatory decisions across regions. Regulators need confidence that results are clinically meaningful beyond one country. Meanwhile, biometrics teams must manage regional differences in patients, medical practice, endpoints, and data quality without weakening the core scientific question. This is where ICH E17, the guideline on multi-regional clinical trials, becomes essential. It helps sponsors design one coherent global study rather than repeating similar trials country by country.
In the context of ICH E17 and global clinical trials, sponsors usually include:
- Pharmaceutical companies developing new drugs, biologics, vaccines, or cell and gene therapies.
- Biotech companies and startups running early- or late-stage clinical programs.
- Medical device companies testing devices, diagnostics, digital therapeutics, or combination products.
- Academic institutions leading investigator-sponsored trials.
- Research hospitals and clinical networks coordinating multicenter studies.
- Nonprofit organizations or foundations funding studies in specific diseases.
- Government agencies supporting public-health or regulatory research.
Why ICH E17 Matters
ICH E17 encourages the use of multi-regional clinical trials under a single protocol. The goal is clear: generate evidence that can support simultaneous or near-simultaneous submissions across regulatory regions. However, global trial design is not just operational expansion. It is a statistical and strategic challenge. Patients may differ by genetics, disease severity, standard of care, diagnostic pathways, adherence, and background therapy. Therefore, the key question is not only: Does the treatment work? The deeper question is: Can the treatment effect be interpreted across regions?
Applying ICH17 to Rare Disease Biometrics
In the orphan drug sector, the “Two-Trial Dogma” is increasingly being replaced by high-fidelity 𝗠𝘂𝗹𝘁𝗶-𝗥𝗲𝗴𝗶𝗼𝗻𝗮𝗹 𝗖𝗹𝗶𝗻𝗶𝗰𝗮𝗹 𝗧𝗿𝗶𝗮𝗹𝘀 (𝗠𝗥𝗖𝗧𝘀), where a single protocol serves as the primary source of evidence for global marketing approvals. While the ICH E17 guideline is often associated with large-scale outcome studies, its core principles are now the operational default for rare disease programs where global recruitment is an absolute necessity.
The Challenge: When a trial enrolls ~80 patients across 15+ countries, achieving local statistical significance in each region is mathematically impossible and brings into question the concept of an MRCT. ICH E17 explicitly acknowledges that MRCTs are planned under the assumption that the treatment effect applies to the entire target population, rather than requiring individual regional significance.
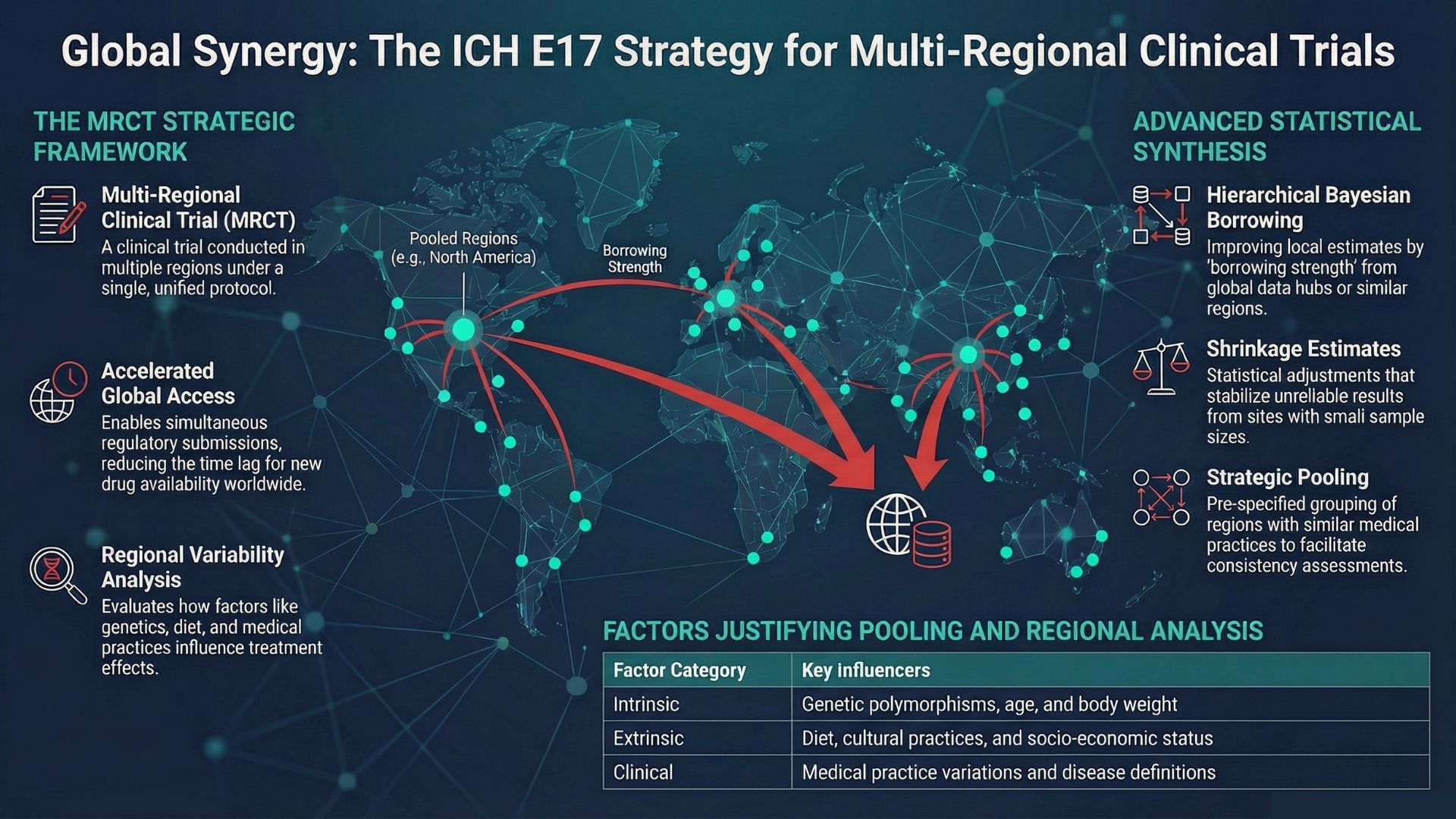
The Biometric Solution: To address small regional cohorts, we implement the “borrowing” and “pooling” strategies outlined in the framework. Pre-specified Pooling: We pool regions or subpopulations (e.g., North American regions or specific ethnic groups) based on shared intrinsic and extrinsic factors to provide flexibility in sample size allocation.
Hierarchical/Shrinkage Models: For regions where sample sizes are too small to support robust estimation, ICH E17 supports borrowing information from other regions using statistical models, such as weighted averages or shrinkage estimates.
Consistency Assesment: So the focus shifts from “testing” for differences which lacks power to evaluating the “consistency of treatment effect,” defined as a lack of clinically relevant differences across the multi-regional population. To ensure data interpretability, we maintain strict adherence to ICH E6 GCP standards and utilize centralized laboratories to minimize regional variability in efficacy assessments.